Historically, the liver has been divided into right and left lobes based on morphological appearance.1 Now, the widley used Couinaud Classification System divides the liver into functional segments.1 Having a good understanding of this classification system is critical for consistent and clear communication between radiologists and surgeons.2 It is also useful for localising findings within the liver. For example, by the end of this article you will hopefully be able to identify which segment the tumour seen in Figure 1 is located in.3 Knowledge of the Couinaud System also helps in understanding the early pathological changes seen in segment 1 during early cirrhosis.
In 1957, a French surgeon, Claude Couinaud, proposed a system for dividing the liver into functional segments. This Couinaud classification is still used today and is based on the orientation of the hepatic veins and portal veins.2
There are three orders of division which result in 9 different segments, with segment 4 being separated into segment 4a and segment 4b. This results in the segments being labelled from 1-8.
The first order of division results in two hemi-livers (which can be referred to as the right and left liver). The second order of division results in four sections (lateral, medial, anterior, and posterior). Lastly, the third order of division divides the four sections in two, resulting in segments 2-8.4 The caudate lobe is classified as segment 1 and is not a part of either the right or left hemi-liver.2
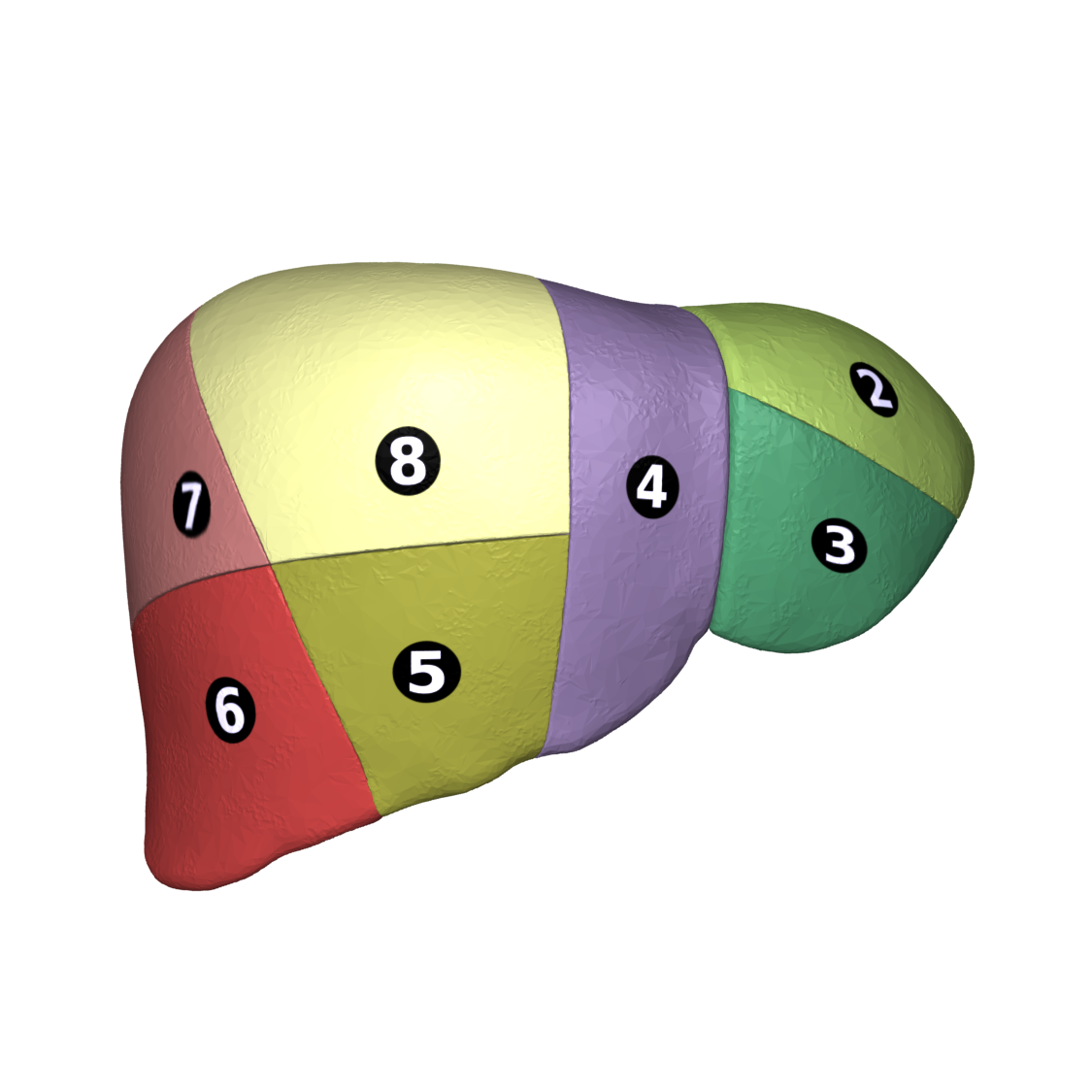
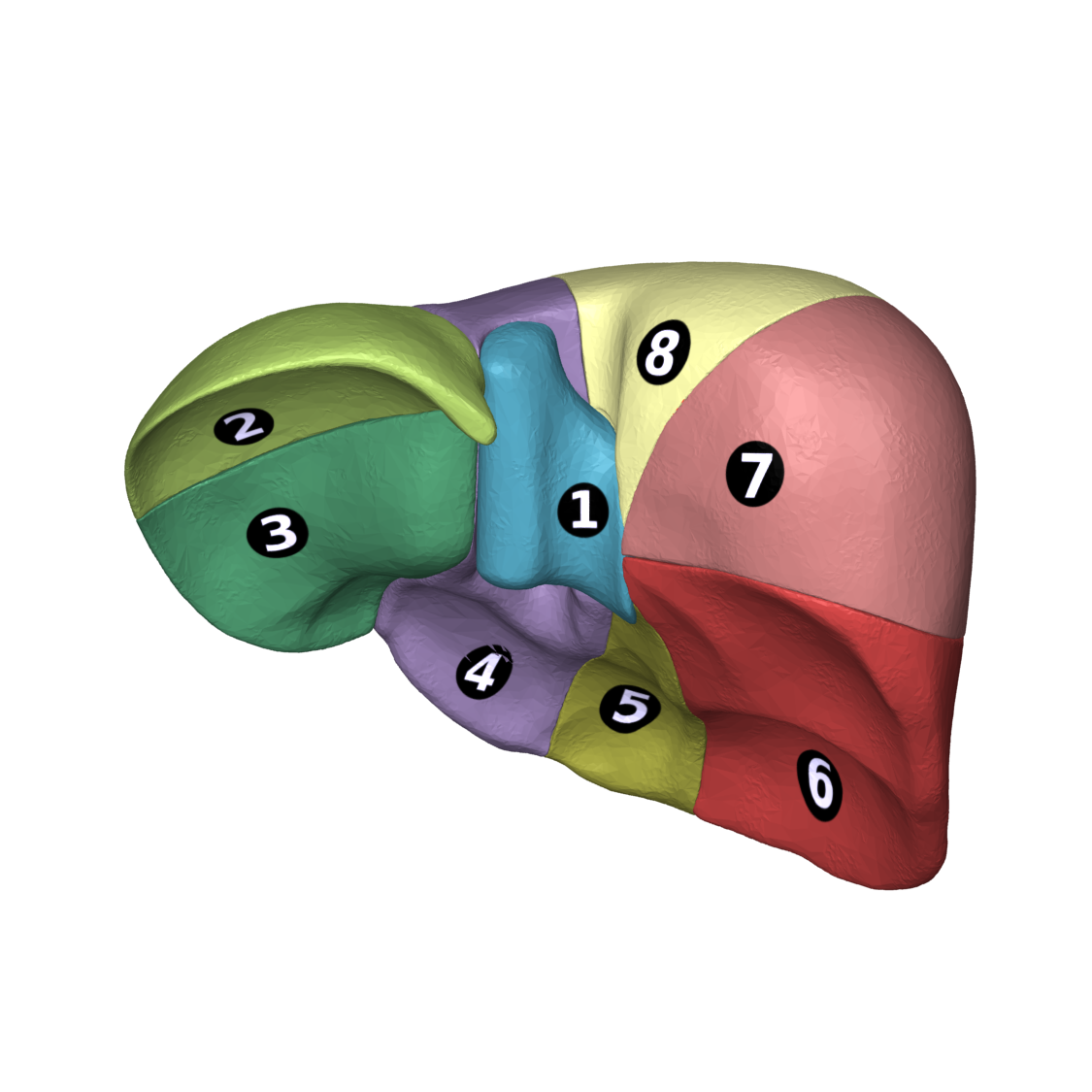
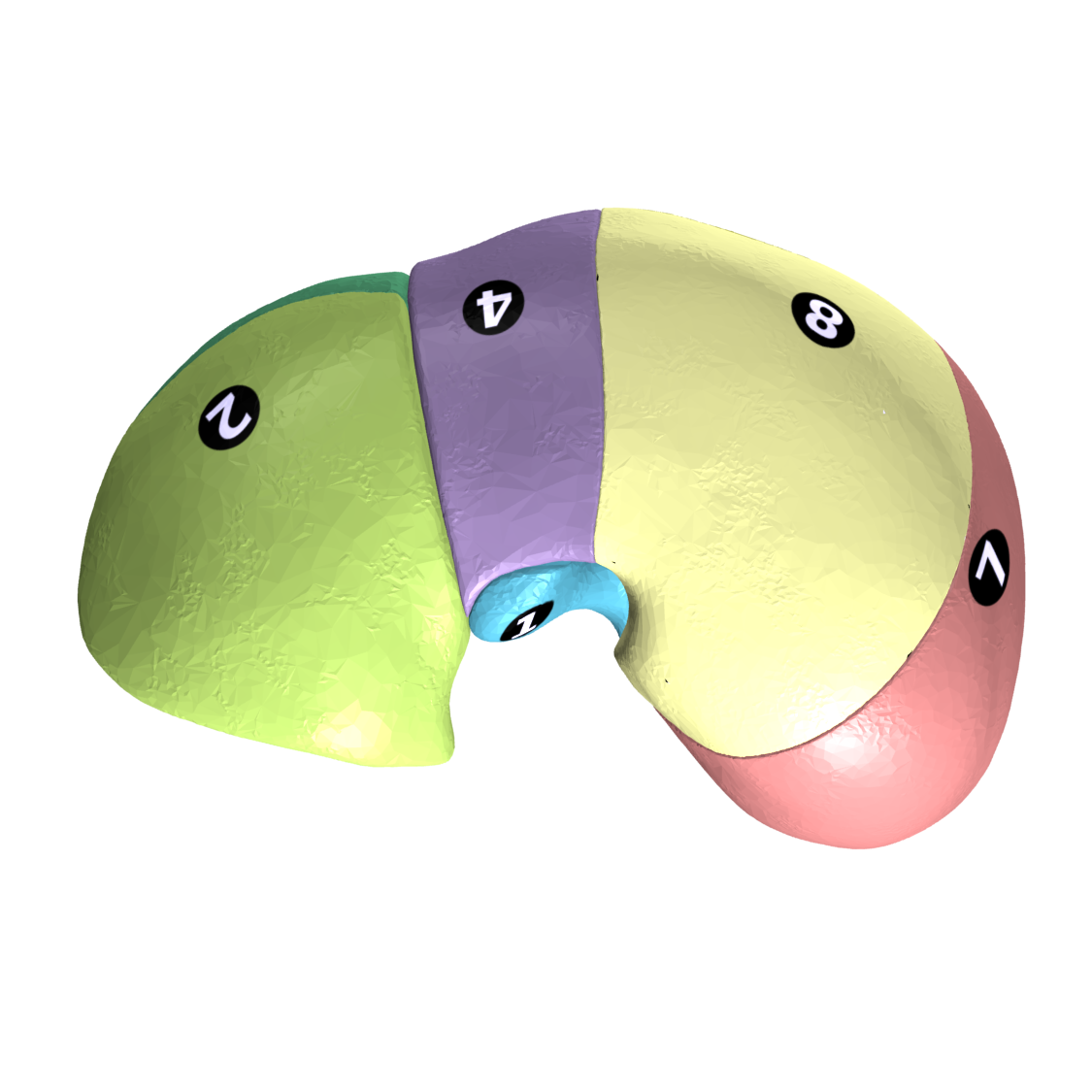
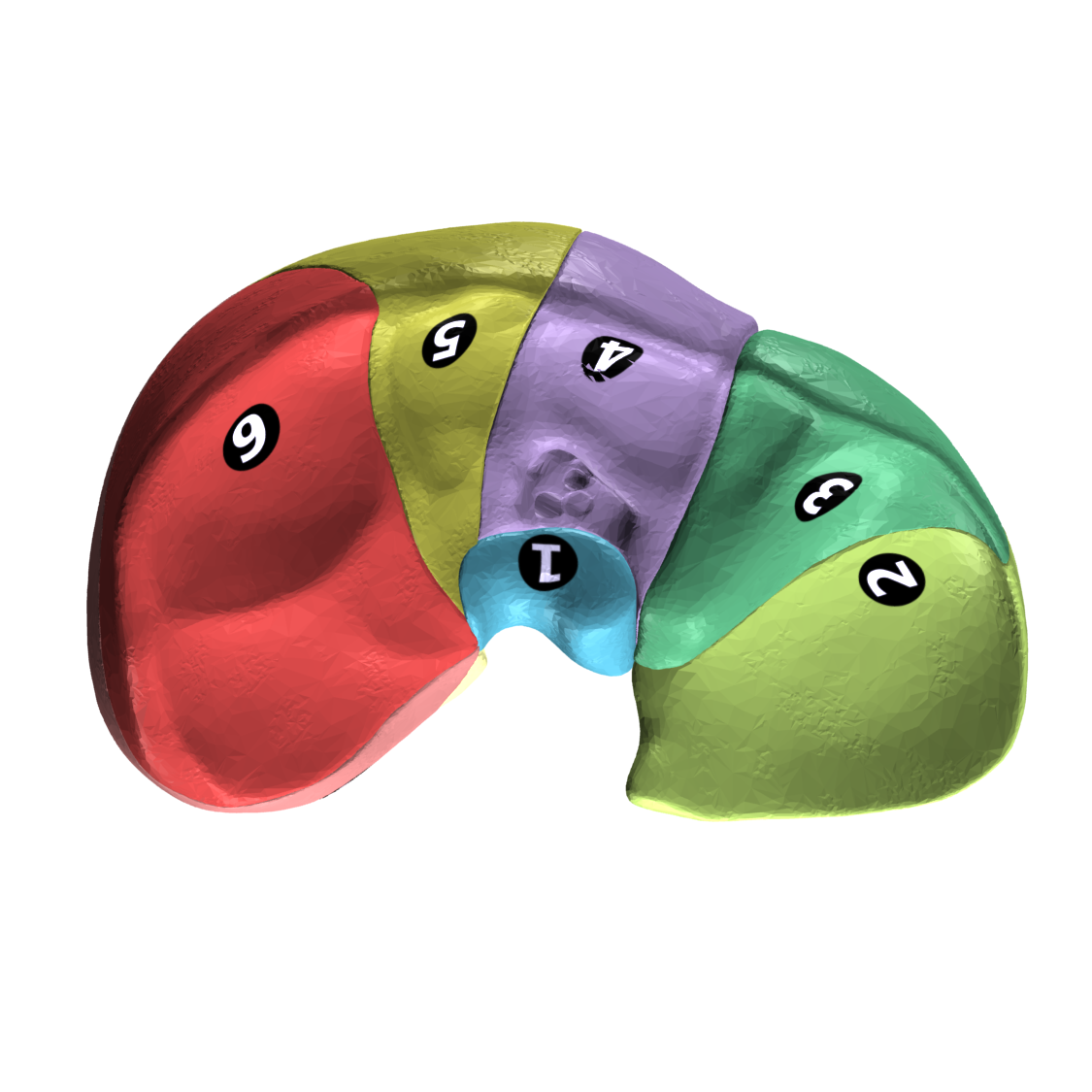
Each individual segment can act independently as each has its own blood supply, venous drainage, and biliary drainage.1 Therefore, this system is also helpful for determining liver resections since one segment can be removed without affecting the function of other segments.5Figures 2-5 show the liver from different views with the segments labelled.6-9
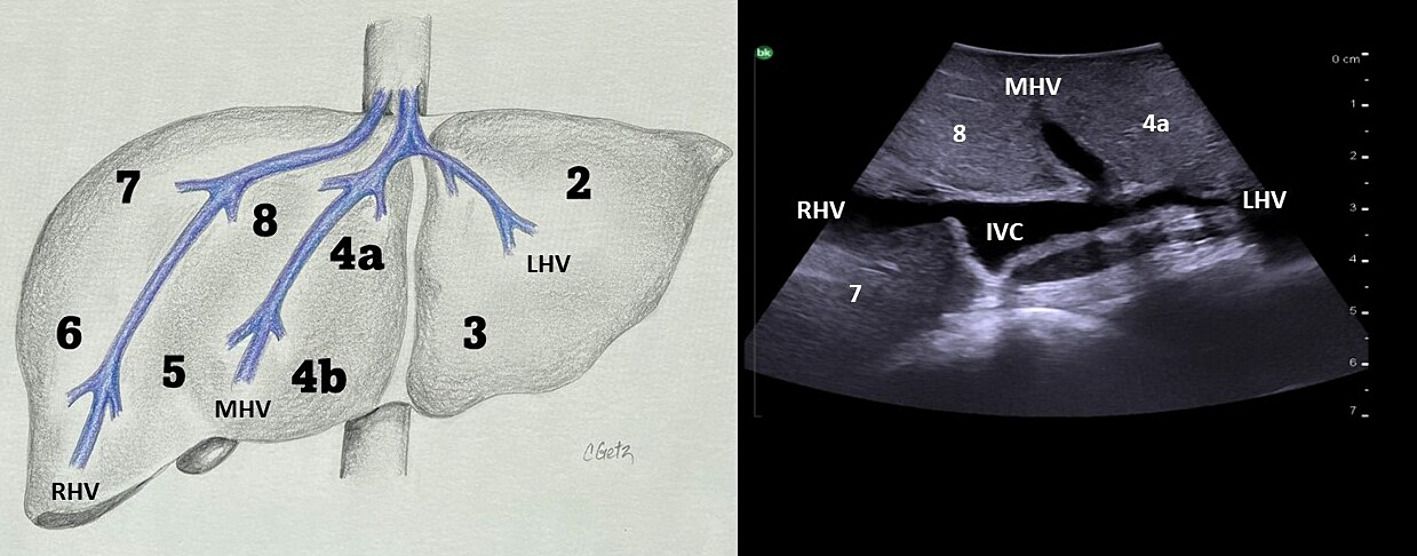
The middle hepatic vein divides the liver into left hemi-liver and right hemi-liver (Figure 6).10, 11
The left hemi-liver contains segments 2, 3, 4a, and 4b.
The right hemi-liver contains segments 5, 6, 7, and 8.
Next, the right hepatic vein divides the right hemi-liver into anterior and posterior sections, while the left hepatic vein divides the left hemi-liver into lateral and medial sections.1,5,10
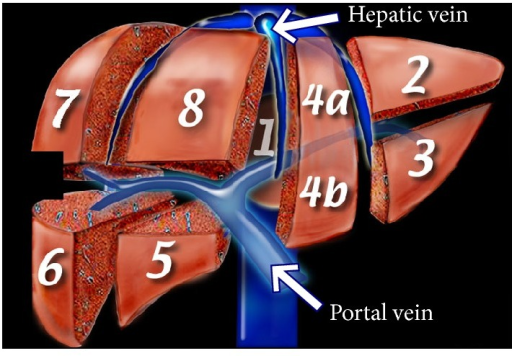
The portal veins are orientated horizontally as shown in Figure 7.12 This horizontal orientation creates what is called the "portal plane" and this divides the sections of the liver (lateral, medial, anterior and posterior) into superior and inferior segments. Remember segment 4 is separated into 4a and 4b).1,5,10
The resulting segments are numbered clockwise, starting from the superior lateral segment, segment 2.
The caudate lobe (segment 1) receives blood supply from the right hepatic artery and can receive blood from both right and left portal veins.
Venous drainage from segment 1 is directly into the inferior vena cava (IVC), which differs from the other segments where venous drainage is into the hepatic veins first. This has clinical significance which is discussed below.
Segment 1 is bound by the fissure for the ligamentum venous anteriorly, the inferior vena cava posteriorly, and the foramen of Winslow inferiorly.
Segment 2
Segment 2 is the superior, left-most segment. It is to the left of the left hepatic vein and superior to the portal plane.
The segments that surround segment 2 are: segment 3 inferiorly and segment 4a to the right.
Segment 3
Segment 3 is the inferior, left-most segment. It is to the left of the left hepatic vein and inferior to the portal plane.
The segments that surround segment 3 are: segment 2 superiorly and segment 4b to the right.
Segment 4
Segment 4 is positioned between the left and middle hepatic veins.
The portal plane divides segment 4 into segment 4a and segment 4b.
Radiopaedia provide a good way of remembering the orientation of these two segments: "4a is above and 4b is below the portal plane".13
The segments that surround 4a are: segment 2 to the left, segment 4b inferiorly, and segment 8 to the right.
The segments that surround 4b are: segment 3 to the left, segment 4a superiorly, and segment 5 to the right.
Segment 5
Segment 5 is the inferior, anterior segment of the right hemi-liver. It is positioned between the right and middle hepatic veins, and inferior to the portal plane.2
The segments that surround segment 5 are: segment 4b to the left, segment 8 superiorly, and segment 6 to the right.
Segment 6
Segment 6 is the inferior, posterior segment of the right hemi-liver. It is to the right of the right hepatic vein and inferior to the portal plane.
The segments that surround segment 6 are: segment 7 superiorly and segment 5 to the left.
Segment 7
Segment 7 is the superior, posterior segment of the right hemi-liver. It is to the right of the right hepatic vein and superior to the portal plane.
The segments that surround segment 7 are: segment 6 inferiorly and segment 8 to the left.
Segment 8
Segment 8 is the superior, anterior segment of the right hemi-liver. It is positioned between the right and middle hepatic veins, and superior to the portal plane.
The segments that surround segment 8 are: segment 4a to the left, segment 5 inferiorly, and segment 7 to the right.
Terminology
The terminology used to define the livers anatomy has been through a confusing and inconsistent history. The International Hepato-Pancreato-Biliary Association (IHPBA) Terminology Committee addressed this confusion by proposing nomenclature in 2000 referred to as the Brisbane 2000 Terminology of Hepatic Anatomy and Liver Resections.2,4 Since then, the proposed terminology has become widespread and is commonly used. It is important to know as it allows clear communication between surgeons, radiologists, and other physicians.
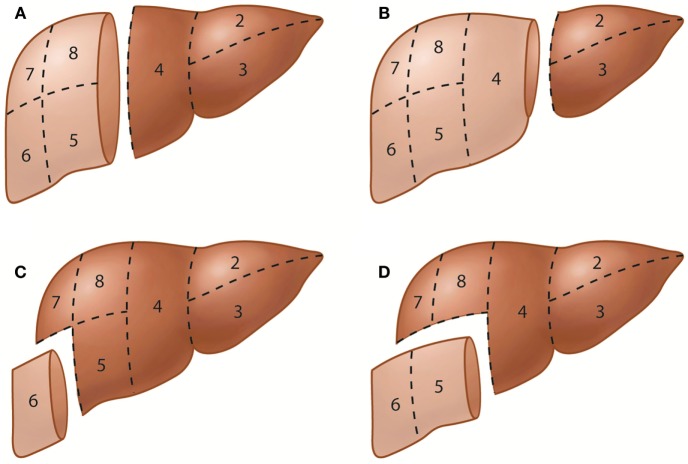
The terminology is based on the Couinaud Classification (discussed above) as each segment can act independently and can be resected without damaging surrounding segments. The terminology proposed by the IHBPA Terminology Committee is shown digramatically in Figure 8 and is discussed below.15
Right Hemi-Hepatectomy
Refers to resection of the right hemi-liver (i.e. segments 5-8).
Left Hemi-Hepatectomy
Refers to resection of the left hemi-liver (i.e. segments 2-4).
Right Anterior Sectionectomy
Refers to resection of the right anterior section (i.e. segments 5 and 8).
Right Posterior Sectionectomy
Refers to resection of the right posterior section (i.e. segments 6 and 7).
Left Medial Sectionectomy
Refers to resection of the left medial section (i.e. segments 4a and 4b).
Left Lateral Sectionectomy
Refers to resection of the left lateral section (i.e. segments 2 and 3).
Segmentectomy
Refers to the resection of any one segment.
Bisegmentectomy
Refers to the resection of any two segments that are in continuity.
Right Trisectionectomy
This is the preferred term to refer to resection of the right hemi-liver (segments 5-8) along with resection of segment 4a and 4b.
Left Trisectionectomy
This is the preferred term to refer to resection of the left hemi-liver (segments 2-4) along with resection of segments 5 and 8.
As you may have noticed, none of the above definitions include resection of segment 1. The convention for relaying the inclusion of the caudate lobe in hepatic resections such as a hemi-hepatectomy or a trisectionectomy is:
By adding, "with resection of segment 1", or alternatively, "extended to segment 1".4
For example, right hemi-hepatectomy extended to segment 1 refers to resection of segments 1, 2, 3, 4a, and 4b.
Since the Brisbane 2000 Terminology, the "New World" terminology has been proposed as an update to the nomenclature and is starting to be seen in the literature. You can read more about the "New World" terminology in this article.
Understanding the segmental anatomy helps localise liver lesions and it also helps understand the physiology behind some pathological findings.
As mentioned above, the caudate lobe (segment 1) drains directly into the inferior vena cava. On the other hand, the other segments drain into hepatic veins before subsequently draining into the inferior vena cava. Because of this, when there is increased venous pressure in segments due to portal hypertension such as in cirrhosis, the segments typically atrophy. The caudate lobe is often spared and hypertrophies as a compensatory mechanism since there is not the same venous pressure as it bypasses the hepatic veins, draining directly into the inferior vena cava.5 This hypertrophy is a specific finding in early cirrhosis, and a caudate lobe to right hemi-liver over 0.65 is especially specific for cirrhosis.5
Common Variants
Named after German Surgeon Bernhard Riedel, Riedel's lobe is an anatomical variation of the liver. There is inferior extension of the right hemi-liver and is often mistaken for hepatomegaly (Figure 9).1,14 This variant is seen in ~5-10% of females and is rarely seen in males.1,14
1. Ramachandran N, Sohaib A. The abdomen and retroperitoneum. In: Butler P, Mitchell A, Healy J, eds. Applied Radiological Anatomy. 2nd ed. Cambridge University Press; 2012:150-180. ISBN 978-0-521-76666-1.
2. Garde, P.S. & Bhute, R.B., 2023. Liver anatomy and cross-sectional imaging techniques: a practical approach. Journal of Gastrointestinal and Abdominal Radiology, 6(3), pp. 089-100. doi:10.1055/s-0043-1767727. License: CC BY 4.0.
3 Fischer, L., Schoebinger, M., Neumann, J.O., Müller, S., Meinzer, H.P., Büchler, M.W., Schmied, B.M., 2008. Does preoperative analysis of intrahepatic venous anastomoses improve the surgeon's intraoperative decision making? Pilot data from a case report. Patient Safety in Surgery, 2, p. 19. DOI:10.1186/1754-9493-2-19. PMID: 18718022; PMCID: PMC
4. Strasberg, S.N., 2005. Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. Journal of Hepato-Biliary-Pancreatic Surgery, 12, pp. 351-355. doi:https://doi.org/10.1007/s00534-005-0999-7.
5. Sun EX, Shi J, Mandell JC. Chapter 2: Gastrointestinal imaging. In: Robinson-Weiss C, Malone FE, Sun EX, Shi J, Jhala K, Matalon SA, eds. Core Radiology: A Visual Approach to Diagnostic Imaging. 2nd ed. Cambridge: Cambridge University Press; 2021:95-228. Volume 1 ISBN 9781108984447; Volume 2 ISBN 9781108984454. doi:9781108966450.
10. Herring, W., 2020. Learning Radiology: Recognizing the Basics. 4th ed. Philadelphia: Elsevier. ISBN 978-0-323-56729-9.
11. Orcutt, S.T., Kobayashi, K., Sultenfuss, M., Hailey, B.S., Sparks, A., Satpathy, B., Anaya, D.A., 2016. Portal vein embolization as an oncosurgical strategy prior to major hepatic resection: anatomic, surgical, and technical considerations. Surgery, 3, p. 14. doi:10.3389/fsurg.2016.00014. PMCID: PMC4786552; PMID: 27014696.
12. Chen Y, Yue X, Zhong C, Wang G. Functional Region Annotation of Liver CT Image Based on Vascular Tree. Biomed Res Int. 2016;2016:5428737. doi:10.1155/2016/5428737. PMCID: PMC5116550. PMID: 27891516.
14. Rocha, J.B.O., de Souza Porto, Í., Tomaz, J.F.M., Araújo, M.M., Mariano, R., Ribeiro, G.A.D.O., Fiuza, V.N., da Silva, A.M., de Araújo Chollet, G.G. & Cerqueira, G.S., 2023. Riedel’s Hepatic Lobe: an anatomical and radiological study. Journal of Morphological Sciences, 40, pp. 511-515. doi:10.51929/jms.40.511.2023.
15. Savopoulos C, Kakaletsis N, Kaiafa G, Iliadis F, Kalogera-Fountzila A, Hatzitolios AI. Riedel's Lobe of the Liver: A Case Report. Medicine (Baltimore). 2015 Jan;94(3):e430. doi:10.1097/MD.0000000000000430. PMCID: PMC4602636. PMID: 25621695.

![Polygon data is generated by Database Center for Life Science(DBCLS)[2]](https://commons.wikimedia.org/wiki/File:Liver_04_Couinaud_classification_anterior_view.png){kind=link}
![Polygon data is generated by Database Center for Life Science(DBCLS)[2]](https://commons.wikimedia.org/wiki/File:Liver_04_Couinaud_classification_posterior_view.png){kind=link}
![Polygon data is generated by Database Center for Life Science(DBCLS)[2]](https://commons.wikimedia.org/wiki/File:Liver_04_Couinaud_classification_superior_view.png){kind=link}
![Polygon data is generated by Database Center for Life Science(DBCLS)[2]](https://commons.wikimedia.org/wiki/File:Liver_04_Couinaud_classification_inferior_view.png){kind=link}